Empowering real estate brokers build visibility and trust through behavioral design
Overview
Pulseara is a SaaS platform designed to help doctors and medical centers manage their daily practice. As the product grew, one operational gap became impossible to ignore: billing.
Doctors were using Pulseara during consultations, but the moment they needed to charge a patient, they had to leave the platform entirely. Some relied on Excel sheets. Others used external invoicing tools, WhatsApp messages, or manual processes handled by assistants.
The result was operational fragmentation:
duplicated work,
disconnected financial records,
inefficient handoffs between doctors and secretaries,
and lost visibility into clinic operations.
I led the end-to-end design of Pulseara’s first integrated billing MVP, from discovery, research and product strategy to usability testing, iteration, roadmap definition, and developer handoff.
The goal was not simply to “add billing.”
It was to integrate administrative operations into the clinical workflow without disrupting how clinics actually work.
TL;DR
Role
Product Designer (sole designer working directly with founders + engineering)
Timeline
~4 months
Responsibilities
Research, strategy, UX, product thinking, usability testing, prioritization, prototyping, developer tickets, roadmap facilitation
Outcome
Billing MVP launched successfully
~30% adoption among active users
Feature became part of Pulseara’s long-term roadmap
Opened expansion opportunities around medical centers
The real problem wasn’t billing
We initially assumed:
Billing was a bigger operational pain point than the team initially expected.
Clinics needed billing and inventory to work together, not as separate systems.
Secretaries and doctors interacted with operational workflows differently.
Ease of use would strongly influence adoption, especially for less digitally fluent users.
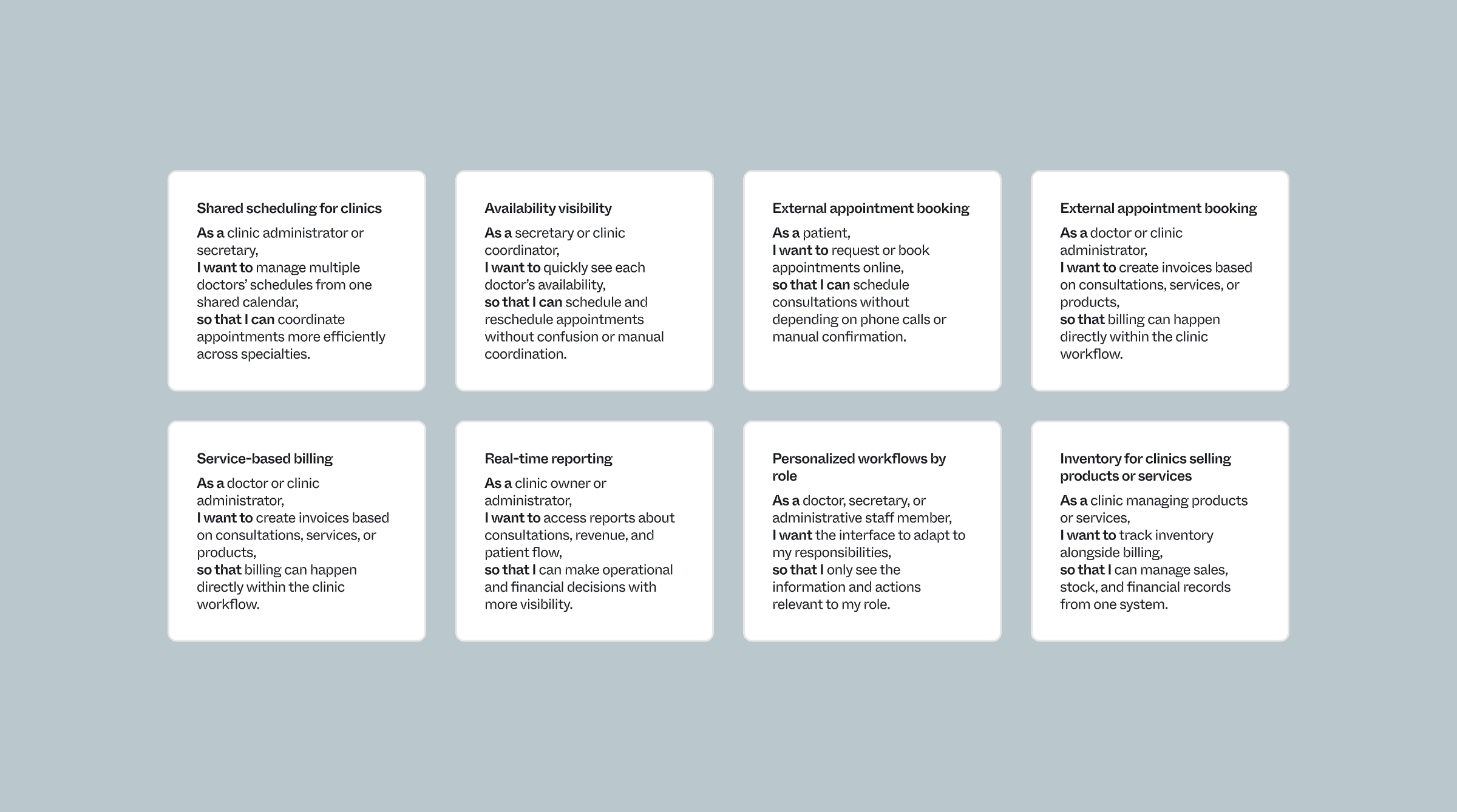
Reality was messier. Through research, multiple product opportunities emerged across for the product roadmap:
scheduling,
telemedicine,
reporting,
permissions,
patient experience,
and operational tooling.
However, billing and inventory management consistently surfaced as the most urgent operational gap due to:
repeated user demand,
high administrative friction,
and direct impact on clinic efficiency and revenue operations.
The challenge was not simply adding invoicing functionality, but designing an integrated operational workflow that could support both doctors and administrative staff without disrupting clinical processes.
Research
Healthcare products often fail when they assume operational workflows behave like traditional SaaS systems.
Clinics don’t operate in clean handoffs.
Doctors sometimes invoice. Secretaries sometimes manage inventory. Administrative staff multitask constantly. And many workflows are still partially manual.
So before opening Figma, I focused on understanding:
who handled what,
where operational bottlenecks appeared,
how information moved across teams,
and which parts of the workflow caused the most mental overhead.
To understand how clinics actually operated, I worked closely with stakeholders, analyzed how competing products approached the problem, spoke directly with doctors and clinic staff, and tested early concepts with real users.
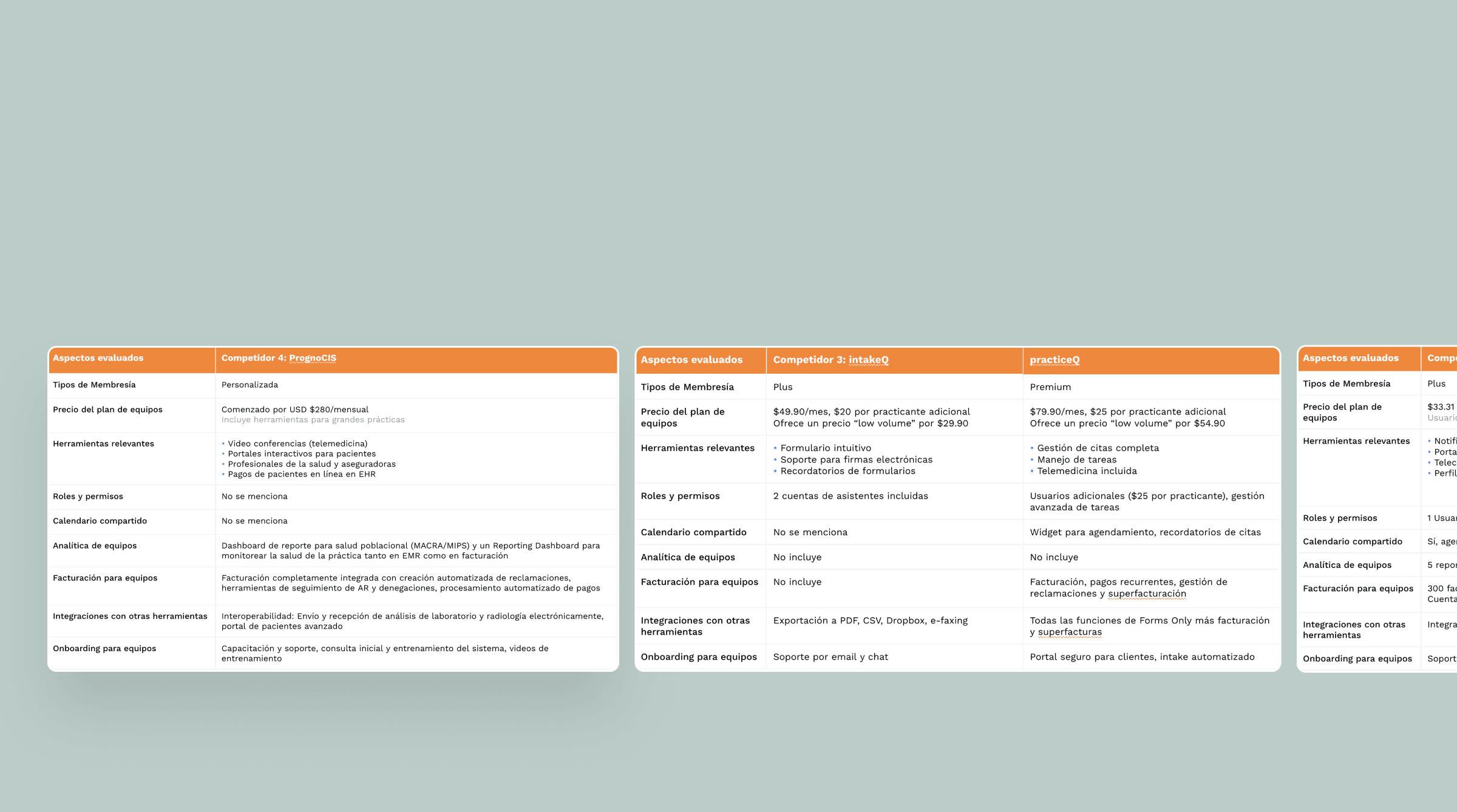
Methodology and techniques
Benchmark
Generative user interviews with 5 users
Recommendation and prioriztion workshop
What we decided to priorizate in the product roadmap?